AI use in U.S. healthcare is high, but adoption is not the same everywhere. About 80% of hospitals use AI in at least one area, yet what that looks like in daily work changes a lot by setting.
If I boil this article down to one point, it’s this: most nonacademic organizations start with AI that saves time, supports billing, and fits inside current workflows. Major academic medical centers can do more because they often have larger budgets, more staff, formal review groups, and in-house data teams.
Here’s the article in plain English:
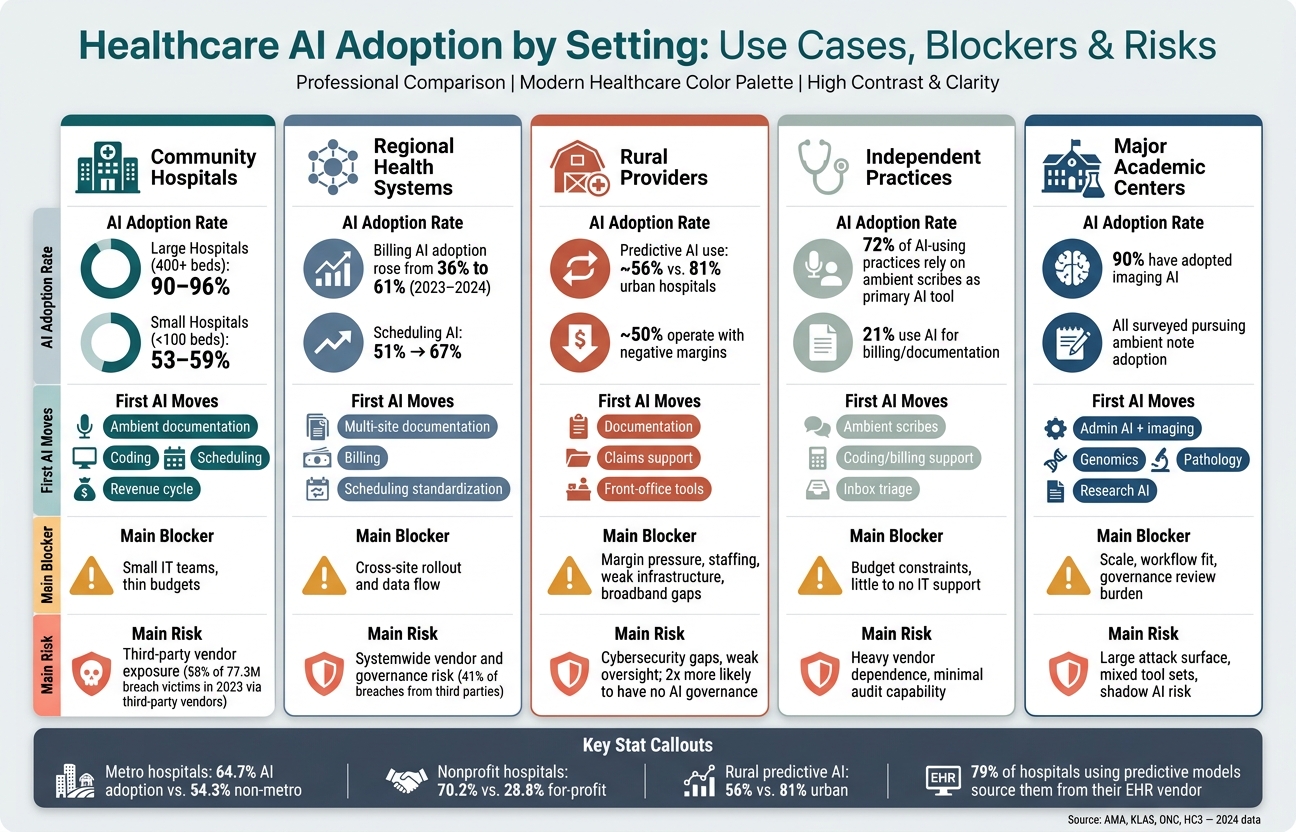
- Community hospitals usually start with ambient documentation, coding, scheduling, and revenue cycle tools.
- Regional health systems focus on standard tools across many sites, but cross-site rollout and data flow are common pain points.
- Rural providers face the toughest limits: thin margins, small IT teams, legacy systems, broadband issues, and weak AI governance.
- Independent practices want one thing first: more time back in the day, so ambient scribes and billing support often come first.
- Major academic centers can go past admin use cases and test imaging, prediction, genomics, pathology, and research-linked AI.
A few numbers make the gap clear:
- Metro hospitals: 64.7% AI adoption vs. 54.3% in non-metro hospitals
- Nonprofit hospitals: 70.2% vs. 28.8% for for-profit hospitals
- Large hospitals (400+ beds): 90%–96% AI use
- Small hospitals (<100 beds): 53%–59%
- Rural hospitals using predictive AI: about 56% vs. 81% in urban hospitals
The article also makes a second point: third-party vendor risk is often the biggest risk. Many hospitals and practices depend on EHR vendors and outside AI companies. That means data sharing, PHI handling, breach exposure, audit logs, clinician review, and contract terms matter from day one.
Before any group expands AI use, the safest first steps are simple:
- Build an AI inventory
- Name one owner
- Track what patient data each tool touches
- Set rules for human review
- Check vendor security, BAAs, retention, and model-use terms
- Create a clear stop process if a tool causes errors or risk
Healthcare AI Adoption by Setting: Use Cases, Blockers & Risks
Healthcare AI Governance - Risks, Compliance, and Frameworks Explained
sbb-itb-535baee
Quick Comparison
| Setting | First AI moves | Main blocker | Main risk |
|---|---|---|---|
| Community hospitals | Documentation, billing, scheduling | Small IT teams, thin budgets | Third-party vendor exposure |
| Regional health systems | Multi-site documentation, billing, scheduling | Cross-site rollout and data flow | Systemwide vendor and governance risk |
| Rural providers | Documentation, claims support, front-office tools | Margin pressure, staffing, weak infrastructure | Cybersecurity gaps and weak oversight |
| Independent practices | Ambient scribes, coding, inbox tools | Budget and little IT support | Heavy vendor dependence |
| Major academic centers | Admin AI plus imaging, prediction, research use | Scale, workflow fit, review burden | Large attack surface and mixed tool sets |
Bottom line: the article shows that AI adoption is not just about interest or access. It mostly comes down to money, staff, infrastructure, governance, and vendor control. If you’re outside a major academic center, the best next move is usually small, low-risk, easy-to-review AI inside current workflows.
1. Community Hospitals
For community hospitals, the capacity gap leads to a pretty simple rule: start with tools that cut staff workload fast. Most of these hospitals aren't chasing sweeping change all at once. They tend to pick a small group of use cases with quick payback. The focus is day-to-day relief, not a full rebuild of hospital operations.
AI Use Cases
A common first step is ambient clinical documentation. AI scribes listen to clinician-patient conversations and create draft notes right in the EHR. That can cut down documentation time and help ease burnout. One health system reported 11% higher physician productivity and 14% more documented HCC diagnoses after deploying ambient AI.[15] By 2025, nearly two-thirds of Epic hospitals were using ambient documentation tools.[6]
Community hospitals are also putting AI to work in revenue cycle automation. About 46% of hospitals and health systems now use AI in revenue cycle management, and 74% have put some type of revenue-cycle automation in place.[17] If you're operating on thin margins, even small drops in denials or faster reimbursement can make a clear difference in cash flow.
Other use cases are picking up steam too. These include imaging workflow support, such as AI-enhanced MRI sequencing that cuts scan times, along with scheduling tools that predict patient volume and help reduce open slots.[10][9]
Operating Constraints
Adoption still varies a lot. Large hospitals with more than 400 beds report AI usage rates of 90% to 96%, while small hospitals under 100 beds are at 53% to 59%.[1][16] The main issue isn't lack of interest. It's capacity.
Smaller IT teams can only handle so many new tools at one time, so rollout usually happens one department at a time instead of across the whole system. Budget pressure adds another layer. Leadership often wants a short payback window before approving a broader rollout.[8][9]
Governance and Risk Structure
Many community hospitals use their current quality, patient safety, or health IT committees to review AI pilots and track denial rates, documentation accuracy, and clinician satisfaction.[9][1] That setup keeps the process practical. Start with a limited pilot. Measure what happens. Expand only if safety and productivity goals stay on track.
When in-house expertise is thin, vendor documentation and ONC/FDA guidance often help fill the gap.[9][1][11]
Cybersecurity and Vendor Dependence
For community hospitals, the biggest exposure tends to sit in third-party risk. About 79% of hospitals using predictive models get them from their EHR developer, and about half also use third-party tools.[13][12] That setup makes sense from a staffing and purchasing standpoint, but it also pushes risk outside the hospital itself.
In 2023, 58% of the 77.3 million people affected by health-sector data breaches were exposed through attacks on third-party vendors. That was a 287% increase over 2022.[14] Ambient AI tools and analytics platforms can add to that risk because they often require patient audio or data to be sent to vendors, which expands the attack surface beyond the hospital's own network.
The limiting factor isn't access to tools. It's the ability to effectively manage third-party risk in a steady way. In practice, that usually means:
- requiring strong business associate agreements
- using standardized risk questionnaires to review encryption and data-handling practices
- monitoring access logs for unusual activity[9][1][10]
Platforms like Censinet RiskOps™ are built for this kind of healthcare third-party risk management, helping organizations structure vendor assessments and keep watch over them over time, even with lean security teams.
As organizations get larger, that same vendor risk gets harder to manage across more sites and workflows.
2. Regional Health Systems
Regional health systems are big enough to standardize AI across many sites, but they usually don’t have the same budget, staff, or research backing as major academic centers. That puts them in an in-between spot. They have more buying power than a small hospital, but the stakes are also higher. If a rollout goes badly, the problem doesn’t stay in one building. It can spread across the whole system.
AI Use Cases
Ambient clinical documentation usually comes first. It fits into existing EHR workflows, and systems can roll it out across sites without a lot of custom build work. In a 2024 survey of 43 U.S. health systems, all were pursuing ambient note adoption, and 90% had adopted imaging AI in some form.[5]
Early results from ambient AI in multi-site systems have looked promising. Some reported about 30% to 34% less after-hours charting and an 8.5% increase in established patient visits.[3][22] Once teams have documentation working in a more standard way, many systems turn to billing and scheduling next.
Operating Constraints
Revenue cycle automation makes sense at the system level when the goal is better billing and scheduling across the enterprise. Between 2023 and 2024, hospital adoption of AI for billing rose from 36% to 61%, and scheduling AI increased from 51% to 67%.[25]
Scale helps, but it also creates friction. A regional system may need to line up hospitals, outpatient clinics, and specialty practices that all work a little differently. That’s where things can snag. The biggest choke point is clean data flow across systems. In practice, tools tend to work best when they sit on top of current workflows instead of forcing a total reset, and when rollout happens in phases with frontline champions leading the way.
Governance and Risk Structure
Regional systems are setting up cross-functional AI governance with leadership from IT, revenue cycle, clinical operations, and compliance. The questions are pretty direct:
- Does the tool code correctly?
- Does it create audit risk?
- Does it cut work for staff, or just pile on more?
Board-level guidance now recommends dedicated AI and cybersecurity subcommittees to deal with model drift, algorithmic risk, and vendor dependencies.[26] That means vendor oversight isn’t just a procurement issue anymore. It becomes a core security job.
Cybersecurity and Vendor Dependence
Most regional health systems depend on EHR vendors and specialized AI companies for ambient scribing, coding support, and workflow automation.[19][20][21] That setup can speed deployment, but it also puts more pressure on oversight.
Third-party vendors account for about 41% of healthcare data breaches, and some analyses estimate that as much as 80% of stolen patient records come from third-party vendors, not hospitals directly.[23][24] When one AI vendor touches dozens of facilities, centralized HIPAA-compliant vendor risk management and continuous monitoring matter a lot. That same vendor-heavy setup gets tougher to control as organizations become smaller and less centralized.
3. Rural Providers
Rural hospitals and clinics are operating with almost no slack. About half of U.S. rural hospitals operate with negative operating margins[36][2], which leaves little room to test new tech and hope it works. That helps explain why AI use trails urban hospitals. Only about 56% of rural hospitals use predictive AI, compared with 81% of urban hospitals[38]. The issue isn't interest. It's budget, staffing, and infrastructure.
Because of that, rural providers tend to focus on a small set of tools that can help right away. Revenue cycle automation and ambient documentation usually move to the top of the list. The reason is pretty simple: cash flow is tight, billing teams are lean, and one physician may cover clinic, inpatient, and ED shifts all in the same day[27][29][7]. In one rollout across 38 rural practices serving 178,536 patients, AI-enabled workflow tools helped address a documented 32.3% primary care provider deficit[33]. When hiring isn't an option, that kind of support can make a big difference.
Governance has to match that reality. Only 32% of critical access hospitals have full EHR functionality, and many still depend on legacy systems, spotty broadband, and small IT teams that can't support always-on AI tools[35]. In practice, rural adoption works best when tools are cloud-based, fit into current workflows, and can be tested in small steps[27][30][4][31].
Rural systems are twice as likely to have no AI governance as their peers[32][39]. So the starting point shouldn't be fancy. It should be simple and clear:
- one accountable owner
- an AI inventory
- an approved-use policy
- a clear way to pause tools when problems show up[28][18][31]
There's another issue here too. Rural populations are underrepresented in many AI training datasets[34]. So providers need to ask vendors direct questions: How was the tool validated? Were rural or medically underserved populations included in that process?[18][4]
The same stripped-down approach applies to cybersecurity. Rural providers are common ransomware targets in part because attackers know these facilities can't easily send patients elsewhere and are under intense pressure to get systems back online fast[18][4]. The U.S. cybersecurity workforce already has a deficit of about 750,000 skilled professionals[40], and small rural facilities often feel that gap the hardest. Practical defenses start with encryption, multifactor authentication, vendor incident response plans, and data-portability exit clauses[18][4][31]. Platforms like Censinet RiskOps™ can help rural organizations structure vendor risk reviews and keep watch over third-party AI tools, even when in-house security capacity is thin.
4. Independent Practices
AI Use Cases
For independent practices, the main goal is simple: get time back.
That’s why ambient scribes have become the anchor use case. Roughly 72% of AI-using practices rely on one as their main AI application.[42][48] These tools listen to the visit, create draft notes in the EHR, and often suggest billing codes and problem lists. The payoff can be big. Two-thirds of users save 1–4+ hours per day on documentation.[48]
That kind of time savings matters when the day feels packed from start to finish.
Use cases don’t stop with scribes. Practices are also using AI for inbox triage, fax processing, patient scheduling, and coding support. AI-assisted coding tools can spot under-coded encounters, and some platforms report recovery of 5–15% in missed revenue.[42][19] The 2024 AMA data points in the same direction: 21% of physicians now use AI for documentation of billing codes and visit notes, up from 13% the year before.[50]
In this setting, AI isn’t mainly about big-system change. It’s about reclaiming hours and helping protect cash flow.
Operating Constraints
Independent practices run lean, and that shapes every AI decision.
Most do not have dedicated IT staff, and capital budgets are often tight. Physicians in private practice already spend only about 27% of their clinical day in face-to-face patient care, with the rest going to documentation, inbox work, and order entry.[45] So when a tool gives time back in a direct, obvious way, it moves to the front of the line.
The practical path is usually cloud-based, EHR-integrated software that can be deployed fast and taught to staff without much friction. In many cases, AI comes through vendors the practice already uses for the EHR, billing, or patient communication.[49][42] That makes rollout simpler, but it also deepens vendor dependence and pushes vendor risk into core workflows.
In other words, governance and vendor oversight aren’t side projects. They become part of daily operations.
Governance and Risk Structure
Most independent practices do not have formal AI committees. Still, someone has to own the work.
Experts recommend naming a single AI governance owner - often the practice manager, physician-owner, or compliance officer - to approve each AI deployment, confirm BAAs are in place, and coordinate staff training.[41][43][46]
At a minimum, practices need:
- An AI inventory
- A HIPAA risk-assessment addendum
- A ban on unapproved consumer AI for PHI
Policy also needs to be plain about one thing: AI-generated notes, codes, and messages must be reviewed by a clinician before use.[43]
Cybersecurity and Vendor Dependence
In independent practices, heavy reliance on outside vendors means cybersecurity risk and procurement risk are basically the same issue.
Any AI tool that processes PHI should be handled like any other ePHI system: with risk analysis, access controls, audit logs, and breach response.[44][47] The basics still do a lot of heavy lifting here - multi-factor authentication, role-based access, and fast removal of access when staff leave.
Before signing with an AI vendor, practices should check a few core items. They should confirm that a HIPAA-compliant BAA is available, find out whether PHI is used to train or fine-tune the vendor’s models, and ask for documentation on encryption and audit logging.[44][47] For practices without in-house security staff, a HIPAA-aligned managed security partner can help cover the monitoring gap.[41][43][44]
That lean, vendor-dependent setup looks very different from the governance-heavy model used in major academic medical centers.
5. Major Academic Medical Centers
Smaller health systems often buy AI tools to cut admin work. Major academic medical centers can do that too, but they can also build, test, and validate those tools in-house.
AI Use Cases
Major academic centers can support a broader AI portfolio because they see more patients, cover more subspecialties, and often have internal data science teams. That changes the equation. It makes sense for them to validate tools that would be hard to justify in many other settings, not just roll them out.
The main clinical use cases still center on workflow: ambient clinical documentation, chart summarization, automated message responses, and denials management. Abridge, for example, has been deployed at major academic centers including UPMC, UCI Health, and Emory Healthcare.[54]
But that’s only part of the picture. Academic centers are also well placed to pilot research-adjacent applications such as sepsis prediction models, pathology image analysis, genomics support, and AI used in clinical trials. They usually have the labeled data, specialist input, and patient volume needed to validate these tools before broader deployment. That difference matters. Nonacademic organizations often adopt AI to save time and protect margins. Academic centers can also use it to generate evidence, train models, and support research workflows.
A broader portfolio sounds great on paper. In practice, it means more systems, more oversight, and more room for things to break.
Operating Constraints
Resources help, but scale gets messy. Academic centers often run multiple EHR instances, varied service lines, and separate research environments alongside day-to-day clinical operations. So a tool that works well in one department can fall apart when rolled out across the enterprise.
If outputs don’t fit into the workflow, clinicians ignore them. At that point, the deployment starts losing its point. KLAS found that lack of governance frameworks, uncertainty around measurable ROI, and difficulty integrating AI into existing systems remain the most common obstacles to broader deployment, even at well-resourced institutions.[56] In plain terms, having the people to build AI is not the same thing as having the systems to scale it.
Governance and Risk Structure
At academic centers, AI governance is usually a formal enterprise function, not a box to check on the way to launch. These organizations use multidisciplinary AI governance committees with formal charters and board reporting.[52]
The Health Sector Cybersecurity Coordination Center recommends structuring these committees with dedicated subcommittees for clinical AI evaluation, cybersecurity, ethics, and vendor and supply-chain risk. It also recommends bringing in finance and revenue cycle leaders when AI touches billing, coding, claims, or prior authorization.[52] AMA policy adds that health care organizations should not use AI systems that introduce overall or disparate risk beyond their ability to mitigate.[55]
That standard carries extra force in an academic setting, where one deployment can affect thousands of patients across multiple sites. These organizations also need formal validation, version control, documentation, and post-deployment monitoring before scaling a tool.
Cybersecurity and Vendor Dependence
The same scale that expands AI use also expands the attack surface. Academic centers store large amounts of protected health information, research data, and intellectual property, which makes them appealing targets. Key threats include data leakage, model poisoning, and prompt injection.[52][37]
Vendor dependence looks different here too. Academic centers often mix custom-built tools, commercial enterprise platforms, and research prototypes. That means procurement terms, data-use rights, model transparency, auditability, retraining limits, and exit planning all need close review.[53] KLAS has found that third-party risk management and asset management remain areas that need work across healthcare cybersecurity programs more broadly.[51] For academic centers, where one vendor model can become embedded across clinical, operational, and research workflows at the same time, that gap creates clinical, operational, and research risk.
Benefits, Tradeoffs, and Risk Controls by Setting
AI can help across almost every care setting in a few clear ways: faster documentation, less admin work, and better coding accuracy. But the payoff doesn't land the same way everywhere.
Outside academic health systems, the value of AI usually comes down to three things: staff, budget, and IT capacity. That’s the part people sometimes miss. The same tool that feels routine in one organization can feel risky in another.
The table below shows how those tradeoffs shift by setting:
| Organization Type | Key Benefits | Primary Tradeoffs |
|---|---|---|
| Community Hospital | Fast ROI from documentation and revenue-cycle tools | Mid-sized IT teams are often stretched thin; interoperability gaps can slow integration |
| Regional Health System | Systemwide standardization and revenue-cycle gains | More systems to govern; inconsistent rollout across facilities can create disruption risk |
| Rural Provider / CAH | Lowest-overhead tools matter most | Financial constraints, staffing shortages, and interoperability failures limit options[58] |
| Independent Practice | Prior authorization automation can save hours per week | Heavy vendor dependence; minimal IT oversight; hard to audit |
| Major Academic Center | Can validate, pilot, and scale more models in-house | Complex governance; shadow AI risk across departments; inconsistent oversight across many pilots |
Those differences shape which controls should come first.
Here’s how common AI tool categories line up with the controls that matter most before and after go-live:
| AI Tool Category | PHI Handling | Vendor Due Diligence | Human Review | Audit Logging | Bias Monitoring |
|---|---|---|---|---|---|
| Ambient clinical documentation | High - draft notes and related conversation content may include PHI | BAA, clear data-flow map, retention and retraining limits | Clinician reviews and signs every note | Session logs, edit tracking, issue reporting | Accuracy and phrasing across patient demographics |
| Revenue cycle and coding | Moderate - claims, diagnosis codes, and supporting documentation | BAA, vendor documentation, denial-pattern transparency | Periodic sampling of coded claims | Denial rate, time to final bill, rework costs per denial | Coding consistency across payer and patient type |
| Imaging workflow support | High - imaging data and metadata can include PHI | Integration specs, validation evidence, workflow fit | Radiologist or ordering clinician final review | Flagged case logs, turnaround metrics | Performance across imaging equipment types and patient populations |
| Inbox and patient messaging | High - symptom reports and patient-reported content can include PHI | Message routing rules, escalation logic | Human triage for high-risk messages | Message classification logs | Escalation rates by message type and patient group |
| Scheduling | Low-to-moderate | Data inputs, model transparency, and vendor documentation | Staff review for flagged appointments | Scheduling change logs | No-show prediction equity across demographics |
Two controls are non-negotiable in every setting: PHI handling and vendor due diligence. If a tool touches patient data, it needs a business associate agreement, a clear data-flow map, and defined retention and retraining limits before go-live[57].
Some organizations use tools built for that process. Censinet RiskOps™ centralizes third-party AI risk management. Censinet AI™ speeds questionnaire collection and evidence summarization. Censinet Connect™ supports shared assessments across vendor relationships.
Human review also has to stay in place for high-stakes outputs. In plain terms:
- Clinicians should review and sign every AI-drafted note.
- Coding teams should audit a sample of AI-generated claims on a set schedule.
- Inbox tools should keep urgent messages and urgent symptom reports in human hands.
The next step is deciding which of these controls nonacademic organizations should put in place first.
What Nonacademic Organizations Can Realistically Adopt Next
Once those controls are in place, the next step is figuring out what nonacademic organizations should adopt first. In most cases, the fastest and easiest wins come from administrative AI. By 2024, about 71% of U.S. hospitals had AI in their EHR workflow.[12][59] But full revenue-cycle deployment still sits at only 20% to 40%.[61] That gap matters because it's where most nonacademic organizations are today.
What does that mean in practice? Keep the first wave narrow. Focus on low-risk use cases that can show a clear return without forcing the organization to rebuild how it works. The rollout tends to look the same almost everywhere: make sure the tool fits inside the current EHR workflow, track one clear metric - like minutes saved, lower denial rates, or net revenue per encounter - and only then expand. Early pilots suggest that coding changes and documentation support can drive measurable revenue gains. The message here isn't complicated: start small, measure carefully, then grow only when the value is plain.
Advanced AI is a different matter. Custom predictive models, large language model deployments, and AI-driven clinical decision support often need mature governance and strong cybersecurity controls that many nonacademic organizations still don't have. Microsoft's rural hospital cybersecurity report found major gaps in email security, MFA, segmentation, and vendor controls.[60] If those basics are still shaky, generative AI is too soon. A simple rule helps: if a small team can't govern it, audit it, and review it fast, it's not ready for that setting.
The table below turns that pattern into a practical rollout plan:
| Setting | Best Near-Term AI Priorities | Biggest Adoption Blocker | Safest Evaluation Approach |
|---|---|---|---|
| Community hospitals | Ambient documentation, coding support, revenue cycle automation, scheduling | Limited IT staff and integration burden | Small pilots in one service line with EHR-embedded tools and finance/quality review |
| Regional health systems | Standardized scheduling, inbox management, prior authorization, multi-site revenue cycle automation | Cross-site governance and interoperability | Central governance with site-by-site rollout and shared metrics |
| Rural providers / CAHs | Documentation, front-office automation, claims support, patient outreach | Cybersecurity gaps and vendor risk | Security-first vendor review, then narrow workflow pilots |
| Independent practices | Ambient scribing, coding and billing support, patient messaging, recall/outreach | Budget and implementation overhead | Low-lift EHR-embedded tools with fast clinician review loops and clear ROI |
Across all four settings, the same pattern shows up: start where governance is easiest to prove. That's the safest place to begin, and usually the smartest. For nearly every nonacademic organization, the next move is pretty clear:
- Build an AI inventory
- Assign an accountable owner
- Document what data each tool touches
- Require a defined review path for errors, bias, and vendor changes
Teams that skip that groundwork often find the holes only after something breaks.
Censinet RiskOps™ centralizes vendor oversight, and Censinet AI™ speeds evidence review for third-party AI risk assessments.
FAQs
Where should a nonacademic provider start with healthcare AI?
Start with a few high-value, low-risk use cases that cut manual work. Good places to begin include documentation, revenue cycle, and patient access. The goal isn’t to do everything at once. It’s to pick a small set of jobs where AI can save time without adding much risk.
Keep the setup simple. For each AI tool, track:
- what the tool does
- what data it uses
- who owns it inside the organization
That basic inventory goes a long way. It gives teams a clear view of what’s in use, where data is going, and who’s on the hook if something goes wrong.
It also helps to build AI checks into the procurement process you already have instead of creating a whole new system from scratch. Use a tiered risk model so not every tool gets treated the same way. A low-risk assistant for internal notes shouldn’t face the exact same review as a tool that touches patient-facing decisions.
Human review should stay in the loop, especially for outputs that affect operations, billing, or patient communication. And if a tool starts missing the mark, there needs to be a plain, workable plan to pause it or shut it down. AI doesn’t get a free pass just because it saves time.
Why do rural and smaller hospitals adopt AI more slowly?
Rural and smaller hospitals often move more slowly with AI. The reasons are pretty straightforward: tight budgets, staff shortages, and limited in-house tech know-how.
On top of that, checking and approving new algorithms can be expensive, often costing around $300,000 to $500,000.
They also have to deal with AI-related risks, including bias and data security, while still running on aging infrastructure. In that kind of setting, urgent clinical demands usually come first, and long-range spending on AI governance gets pushed down the list.
What vendor risks should healthcare organizations check first?
Start by making a full list of every AI tool in use, then rank each one by risk. Put extra weight on three things: patient safety, PHI exposure, and how much work the tool does on its own.
Then look past the usual security checklist. Find out how the model was trained, what data it relies on, and how the vendor deals with bias. Your contracts should also require notice before any retraining or major model change. And every tool needs a clear internal owner who can approve it, watch it over time, and shut it down if something goes wrong.
