AI attacks in healthcare don’t start and end with one bad click. I’d treat them as a five-stage path that can touch chatbots, imaging tools, EHR-linked assistants, billing systems, and vendor platforms.
Here’s the short version:
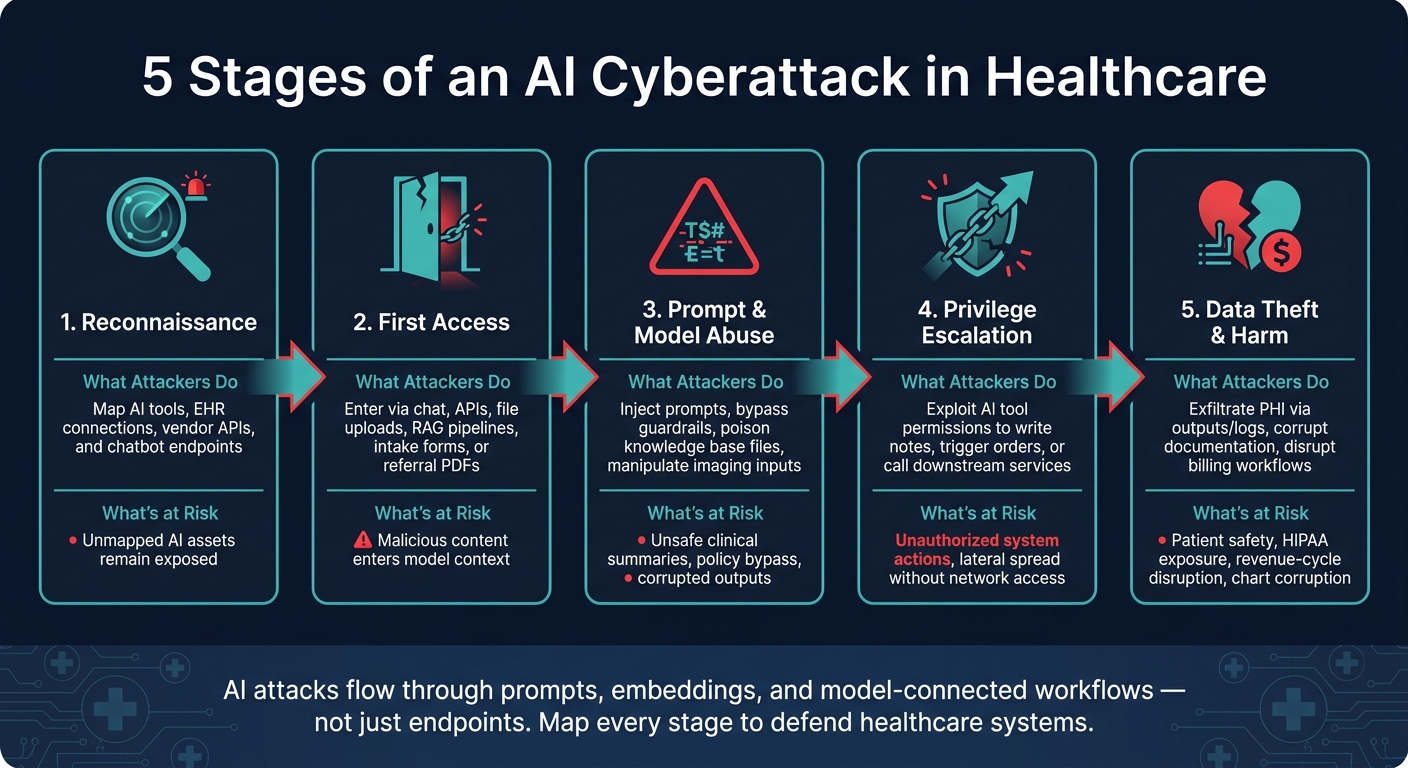
- Stage 1: Reconnaissance - an attacker maps which AI tools you use and how they connect to systems like the EHR, PACS, scheduling, and claims.
- Stage 2: First access - they reach the model through chat, APIs, file uploads, RAG sources, or third-party tools.
- Stage 3: Prompt and model abuse - they try prompt injection, poisoned files, or crafted inputs to change model behavior.
- Stage 4: Escalation - they use AI permissions, tool use, or trusted output to affect other systems or staff actions.
- Stage 5: Data theft and harm - PHI leaks, bad charting, claim errors, care delays, and revenue loss start to show up.
What stood out to me is this: the attack may never look like a normal endpoint breach. Instead, it can flow through prompts, embeddings, logs, retrieval content, and model-connected workflows. In healthcare, that means the blast radius can hit privacy, patient safety, and money at the same time.
A few points matter most:
- Untrusted input is the weak spot. A patient message, PDF, policy file, image, or referral note can carry hidden instructions.
- Third-party vendor risk management is critical because vendor AI adds blind spots. If you can’t trace where data goes and what the tool can trigger, you can’t judge risk well.
- Logging needs to cover AI-specific evidence. That includes prompts, outputs, tool calls, config changes, retrieval events, and API activity.
- HIPAA risk can show up in places teams miss. Think inference logs, vector stores, and model training or tuning paths.
- Stage mapping helps teams act sooner. It gives security, IT, privacy, compliance, and clinical leaders a shared way to review controls and response steps.
| Attack stage | What I’d watch for | What could go wrong |
|---|---|---|
| Reconnaissance | Probing queries, endpoint discovery, vendor API testing | Hidden AI assets stay exposed |
| First access | Odd file uploads, external API use, strange chatbot inputs | Bad content enters model context |
| Prompt/model abuse | Prompt probing, guardrail bypass attempts, unsafe outputs | Wrong summaries, unsafe advice, policy bypass |
| Escalation | Unexpected tool calls, note writes, downstream task triggers | System-to-system spread |
| Data theft and harm | PHI in outputs, log leaks, billing changes, care workflow issues | Privacy events, chart corruption, claim trouble |
If I were summarizing the article in one line, it would be this: you need an AI asset list, stage-by-stage controls, and AI-aware incident response before AI risk spills into patient care or billing.
That’s the lens I’d use for the rest of the piece.
5 Stages of an AI Cyberattack in Healthcare
AI Cybersecurity Risks and Compliance for Healthcare Organizations
sbb-itb-535baee
The stages of an AI attack in healthcare environments
The five-stage attack path gets easier to understand when you look at how it shows up in day-to-day healthcare work. Each stage points to a place where controls can fail.
| Stage | What the attacker does | Healthcare example | Primary defender concern |
|---|---|---|---|
| Reconnaissance | Maps AI systems and workflows | Finds chatbot, imaging AI, and vendor copilots | Unmapped AI endpoints and unmanaged access paths |
| First access | Reaches AI through chat, API, RAG, or files | Poisons a PDF or embeds instructions in a patient message | Untrusted content entering the model's context |
| Prompt/model abuse | Manipulates instructions or bypasses safety rules | Forces an unsafe clinical summary or dodges guardrails | Corrupted clinical output and policy bypass |
| Privilege escalation | Leverages AI permissions or tool access | AI writes notes or triggers downstream tasks | Unauthorized actions and lateral system impact |
| Exfiltration and impact | Extracts data or disrupts operations | PHI leak, corrupted documentation, workflow disruption | Patient safety risk, privacy exposure, and revenue-cycle harm |
Stages 1 and 2: Reconnaissance, AI discovery, and first model access
The first thing attackers do is look for what they can see and what they can reach.
Stage 1 is about mapping the AI systems a health system uses and seeing how those systems connect to EHRs, patient portals, and vendor tools. In plain terms, that might mean probing a hospital website’s triage chatbot to check whether it pulls from EHR data, testing a portal’s virtual assistant for signs of backend access, or querying a vendor API to figure out what model sits behind the service.
Stage 2 is where that knowledge turns into access. And the number of possible entry points is often bigger than teams expect. RESTful APIs and FHIR endpoints tied to mobile apps, RAG pipelines pulling from document repositories, and embedded copilots inside clinical systems can all open the door. Indirect paths matter too. Intake forms, referral PDFs, and third-party feeds can carry hidden instructions that the model later reads and uses. If that sounds small, it isn’t. Any one of those paths can turn into a patient safety or privacy issue if the model acts on a malicious payload.
That’s why a living inventory of AI endpoints matters. If your team doesn’t know which systems take free-text input, where files can be uploaded, or which APIs are reachable from outside, the Stage 1-2 gap stays open.
Stages 3 and 4: Prompt manipulation, model abuse, and privilege escalation
Once attackers get in, the job changes from discovery to control.
The most visible method is direct prompt injection. An attacker enters crafted instructions into a chatbot or staff assistant and tries to override safety rules or push the model into producing unsafe clinical output. Indirect prompt injection is tougher because the malicious instruction is buried inside a clinical note, a PDF, or a RAG knowledge base entry that the model pulls in and follows on its own.
Indirect prompt injection is often the more dangerous variant because attackers can hide payloads in content the AI is expected to trust and ingest automatically.
Recent studies show imaging models can also be manipulated through embedded instructions and poisoned inputs.[8][9]
Stage 4 is where bad output starts turning into system access. If the AI can read records, write notes, trigger orders, or call services, a manipulated response can move straight into action. That’s the jump from a corrupted chatbot answer to damaged documentation or an automated downstream task, without the attacker ever touching the network in a direct way.
Stage 5: Data exfiltration and impact on clinical and business operations
Stage 5 is where the damage becomes visible in the real world. At this point, attackers usually want one of two things: data or disruption.
On the data side, a compromised AI system can become an exfiltration channel. PHI can leak through chat responses, API outputs, or logs. Model inversion and theft techniques use crafted queries and stolen artifacts to reconstruct or approximate proprietary models and datasets.[4][5] In healthcare, that can expose de-identified, or even re-identifiable, patient records used in training. A healthcare compliance guide notes that PHI entered into or generated by a generative AI tool can still be treated as PHI, and that a provider may not realize an impermissible disclosure occurred when using the wrong environment or configuration.[7]
On the operations side, the effects can hit fast. Manipulated documentation tools can insert or omit allergy information, code status, or medication changes.[2][6] That can corrupt the medical record and set off prescribing and coding errors. Compromised billing models can misclassify claims,[3][1] which can lead to denials, audit exposure, and revenue-cycle disruption. The end result is patient safety risk, compliance exposure, and harm to the revenue cycle.
These stages tend to show up most clearly in patient-facing tools, clinical AI, and workflows tied to outside vendors.
Healthcare scenarios that make each attack stage easier to recognize
Patient-facing and staff-facing LLM workflows
These stages are easier to spot when you look at everyday hospital workflows. A public symptom-checker chatbot, for example, is usually easy to find and test. It often doesn't need a login, and it may connect to patient education pages or scheduling systems. An attacker probing a Virtual Nurse chatbot might begin with meta-questions to map its integrations, then shift to prompt injection after the model and its retrieval links come into view.
Testing of clinical chatbots has shown that prompt injection can expose system instructions and backend details.[12] If a hospital policy site is indexed for retrieval, a malicious file can slip in instructions that the assistant later repeats or follows. That can expose policy text, prior case examples, or unredacted PHI stored in the knowledge base.
Imaging AI and clinical decision support systems
Imaging and decision-support tools follow a different pattern. An attacker may find an imaging AI service through public documentation, then start testing its upload path with malicious inputs. If someone gets access to that upload path, they can submit slightly altered images or hide pixel-level instructions that skew the model's output and slow triage.[10][11] The big issue is straightforward: when imaging AI helps drive triage, a manipulated result can push urgent studies down the line.
Vendor AI services and connected hospital workflows
Managing third-party AI risk is often the hardest path for defenders to see. Third-party AI tools can create the most tangled attack paths because they sit between multiple hospital systems and opaque outside dependencies. The Change Healthcare incident showed how one vendor failure can disrupt prescriptions and claims across the country.[13] If defenders can't trace the flow of data into and out of the vendor, they won't know where an attack starts or where it ends. They need a clear map of what data goes in, what the vendor sends back, and which workflows those outputs can touch. That map is what supports the controls, monitoring, and governance decisions covered next.
How mapping attack stages improves defense and governance
Knowing the stages helps teams put the right controls in the right places, assign clear owners, and keep an eye on risk. That takes AI risk out of the abstract and turns it into something teams can track and manage day to day.
Stronger risk assessments and third-party oversight
Once teams understand the stages, they can turn them into review questions. Look at where untrusted text or files come in, which systems handle PHI, what logs exist, and how fast risky features can be shut off.
Those questions matter for both internal tools and vendor services. For third-party AI products, they should show up in pre-procurement questionnaires and contract terms. Contracts should spell out a few non-negotiables:
- No use of customer PHI for model training without written approval
- Support for customer-controlled logging
- Defined response times and escalation paths for AI-specific incidents
It also helps to map each stage to risk entries, owners, frameworks, and playbooks. That makes AI risk visible and traceable instead of letting it disappear into a broad IT risk bucket. [15]
Clearer monitoring signals and a structured incident response
The same stage map shows defenders what to watch for and how to act. Early on, watch for unusual AI access, probing queries, and prompt probing - repeated attempts to expose instructions or get around guardrails. In later stages, shift attention to unexpected tool calls, spikes in sensitive data retrieval, and responses that drift from approved behavior. [15][16]
If an incident happens, the stage framework gives the response team structure. Containment should match the stage. For prompt abuse, disable tool calls. For suspected exfiltration, revoke keys and isolate integrations. Evidence collection should include prompt histories, output logs, tool call traces, and configuration snapshots, all with proper PHI handling. Privacy and clinical leaders should be involved early to judge PHI exposure and any effect on care, orders, or documentation. [15][17][18]
The NIST AI RMF 1.0 treats response, recovery, and communication as baseline AI requirements. [14]
Governance workflows with Censinet
Mapping attack stages works best when it lives inside a formal governance process instead of a one-time review. Censinet RiskOps™ brings AI risk data into one place across internal and third-party assets, including model type, PHI exposure, clinical criticality, and vendor relationships. Teams can tag assessment findings by stage, which helps governance committees spot where vendors lack enough logging or where containment measures are weak.
Censinet AI™ can summarize vendor responses, flag gaps in logging, PHI use, and containment, and map findings to attack stages. It also adds human review at key points, sending findings and tasks to the right stakeholders - including AI governance committee members - for approval before anything moves forward.
That same stage map then feeds straight into ongoing governance and review.
Conclusion: Turn AI attack stage awareness into a healthcare risk program
AI attacks don’t happen all at once. They unfold in stages. When defenders map those stages, they have a better shot at stepping in early, limiting damage, and cutting patient safety, privacy, operational, and regulatory risk before it spreads. That’s why inventory and stage mapping should come first.
Start with an AI inventory. List each system, its owner, the data it touches, and the workflows it connects to. Then map every system to the stages where it’s most exposed and the controls most likely to fail. From there, you can focus fixes where they matter most, especially for chatbots, documentation tools, and imaging AI. The point isn’t to make paperwork look neat. It’s to use that map to guide risk decisions.
Those findings should flow into third-party risk, the enterprise risk register, and governance workflows. A stage-based risk entry gives leadership a clearer picture of where AI creates material exposure and which controls need attention first.
The NIST AI RMF fits well with healthcare governance, and logging prompts, outputs, tool calls, data access, and administrative changes helps with detection, incident response, and vendor oversight.[19][20][21][22] That’s the kind of structure that keeps oversight steady as AI use grows.
Censinet RiskOps™ and Censinet AI™ keep findings in one place and route them to the right stakeholders for day-to-day oversight. Together, they turn stage awareness into continuous action.
FAQs
What counts as an AI asset in healthcare?
In healthcare, an AI asset is more than standard IT infrastructure. It covers the full AI lifecycle, including training and tuning data, model weights, checkpoints, and development software artifacts.
That also includes clinical interfaces like chatbots and documentation tools, along with connection points such as APIs, FHIR and HL7 connectors, and cloud-based vendor services.
Put simply, if a system or dependency processes inputs in a way that shapes clinical or business workflows, it counts as an AI asset.
How is an AI attack different from a normal breach?
An AI attack is different from a normal breach because it shifts behavior quietly instead of leaning on old-school intrusion, malware, or account takeover.
Instead of going after infrastructure, it targets a model’s logic, training data, or input channels to steer outputs in the wrong direction. And because it can move through allowed channels - like standard API calls or routine clinical data inputs - it may slip past alerts while still affecting clinical results, diagnostic accuracy, or treatment recommendations.
Which AI attack stage should teams focus on first?
Healthcare teams should start with the data and training pipeline. That’s where the biggest risk begins.
If attackers poison training, tuning, or retrieval data, they can slip in malicious logic or hidden backdoors before the model ever goes live. And once that happens, the damage is much harder to spot.
Protecting data provenance and upstream pipelines gives teams a better shot at stopping problems early, when they’re still easier to control, instead of dealing with them after the model is live and producing outputs.
