If you work in U.S. healthcare, the best choice is usually simple: use a pre-built framework when you need audit alignment and outside validation, build custom controls when your cloud setup is hard to fit into a standard model, and combine both when you need each.
Here’s the short version:
- Pre-built frameworks like NIST CSF, NIST SP 800-53, and HITRUST CSF help you move with more structure.
- Custom frameworks fit hybrid cloud, legacy clinical systems, research data flows, and AI use cases more closely.
- Hybrid cloud is now common: 73% of organizations run hybrid estates.
- Third-party risk is a top issue: 44.5% of initial access vectors in late 2025 came from third-party software-based entry.
- AI governance gaps matter too: 63% of breached organizations in 2025 lacked AI governance policies.
- Cost matters: HITRUST can run from $30,000 to $400,000+, plus $15,000 to $40,000 per year for MyCSF.
- Time matters: custom programs often take 9–18 months to fully put in place.
If I had to boil the article down to one point, it would be this: pick the model your team can map, run, prove, and keep up over time. In healthcare, that means looking at compliance needs, cloud sprawl, vendor risk, internal staffing, and how much variation exists across clinical and business systems.
Cloud Compliance Explained: SOC 2, HIPAA, PCI-DSS & GDPR Guide
sbb-itb-535baee
Quick Comparison
| Criteria | Pre-Built Frameworks | Custom Frameworks |
|---|---|---|
| Best use | Audit alignment, standard governance and metrics, vendor assurance and vendor risk management | Hybrid cloud, legacy systems, research, AI, edge cases |
| Setup time | Faster start | Longer build time |
| Flexibility | Lower | Higher |
| Staffing need | Lower internal lift | More engineering and security lift |
| External recognition | Strong | Limited unless mapped to known standards |
| Cost pattern | License, audit, certification costs | Internal build and upkeep costs |
| Cloud fit | Often needs overlays | Built around your stack |
| Best choice for many healthcare teams | Good baseline | Good add-on for special cases |
So if you want the simplest takeaway: start with a known baseline, then add custom controls where your cloud, data, or clinical workflows do not fit cleanly.
Pre-built cloud security frameworks: what they offer and where they fit
Pre-built frameworks come from known standards groups and healthcare programs. They give teams a set structure for risk, ownership, and evidence.
This option makes the most sense when speed, outside trust, and repeatable controls matter more than building something custom. In practice, these frameworks play different roles across governance, assurance, and technical control.
Pre-built frameworks commonly used in healthcare cloud programs
Three frameworks show up again and again in U.S. healthcare cloud programs, and each one does a different job.
NIST CSF 2.0 is a governance framework. It focuses on outcomes and stays technology-agnostic. It organizes security work into six functions: Govern, Identify, Protect, Detect, Respond, and Recover. Healthcare teams often use it to connect security priorities to enterprise governance. The tradeoff is simple: it doesn't spell out specific technical controls, so teams usually pair it with more detailed implementation guidance. Best for governance and prioritization.
HITRUST CSF is a healthcare-focused assurance framework that pulls together requirements from HIPAA, NIST, ISO, and PCI into one certifiable control set. That can cut down on audit duplication and help with vendor assurance. In cloud setups, vendors can inherit much of the infrastructure-layer testing from cloud providers, which cuts some of the manual assessment work. Best for assurance and vendor reporting.
If your team needs a more prescriptive control baseline, NIST standards are often where you turn. NIST SP 800-53 lays out prescriptive technical controls for high-rigor settings, including FedRAMP-aligned programs. NIST SP 800-66 shows how to apply the HIPAA Security Rule through NIST risk management. Best for prescriptive control implementation.
Strengths and limits of pre-built frameworks
The biggest upside is speed. Teams don't have to build the framework, assessment criteria, or documentation templates from scratch. There's also a trust factor here. Regulators and enterprise buyers already know these frameworks, so certifications like HITRUST carry weight with payers, providers, and regulators.
But there are tradeoffs, and some of them hit hard. Control overload is common. A small digital health team can end up dealing with 100+ requirements that don't fit its setup [1]. HITRUST certification can also get expensive fast, with costs ranging from $30,000 to $400,000+ depending on the assessment tier and the size of the organization, plus an annual MyCSF subscription of $15,000 to $40,000 [4]. And rigid models don't always fit messy healthcare reality, especially with legacy device integrations and odd clinical workflows.
Here’s how those tradeoffs usually play out across speed, cost, compliance, and cloud depth:
| Advantage | Constraint | Healthcare Impact |
|---|---|---|
| Faster starting point | Too many controls | Speeds up cloud adoption but may force small teams to manage 100+ unnecessary controls [1] |
| Standardized assessment | High certification costs | Simplifies third-party vendor vetting for HDOs; HITRUST r2 can reach $400,000+ for large enterprises [4] |
| Strong external signaling | Limited flexibility | Builds immediate trust with payers and partners; may struggle to adapt to legacy device integrations [2] |
| Control inheritance | Reliance on provider evidence | Reduces infrastructure assessment burden but requires trust in provider-provided evidence [3] |
So the real issue isn't whether pre-built frameworks are good or bad on paper. It's whether their speed and outside trust are worth the cost, scope, and fit issues in your cloud environment.
Custom-built cloud security frameworks: when building your own makes sense
A custom-built cloud security framework pulls selected controls from standards like HIPAA, NIST, HITRUST, and CIS into an internal model shaped around your architecture, workflows, and risk tolerance. Instead of adopting a pre-built framework end to end, you build a model that matches what your environment actually looks like.
This approach makes sense when pre-built frameworks feel too rigid for hybrid, legacy, or research-heavy environments. That usually shows up in places like health systems running hybrid clouds, organizations connecting legacy clinical systems, or research teams moving sensitive data through AI pipelines. As of 2026, 73% of organizations operate hybrid cloud estates [1], which makes a single generic control set harder to apply across every workload.
How custom frameworks are typically built
The process usually starts with a HIPAA-aligned risk analysis based on the actual clinical setting. From there, teams pull in NIST CSF 2.0 for governance structure, NIST SP 800-53 for deeper control detail, and CIS Benchmarks for hardening guidance, then map those controls to live workloads.
On the technical side, the foundation often includes:
- Identity and access controls such as SSO, MFA, RBAC, and break-glass access
- Encryption and tokenization plans shaped to specific data types
- Workload segmentation through account boundaries and VPC/VNet isolation
- Centralized logging tied to clear asset ownership
It also helps to build controls into landing zones and infrastructure as code, so new environments inherit the baseline by default instead of relying on teams to set everything up by hand.
Good custom frameworks also set clear ownership across security, compliance, and clinical teams. That matters for a simple reason: when something goes wrong, people need to know who decides, who fixes it, and who accepts the risk.
Strengths and limits of custom frameworks
The main upside is fit. A custom framework can separate PHI workloads from lower-trust research environments, support medical device integrations and legacy systems, and address untracked data movement in AI pipelines that generic frameworks often miss. That gap is getting harder to ignore. In 2025, 63% of breached organizations lacked specific AI governance policies [1].
But the tradeoffs are real. Full implementation usually takes 9–18 months [4], needs dedicated in-house expertise across security and clinical domains, and adds a steady documentation load.
The tradeoffs stand out most when you compare fit, automation, cost, and governance side by side:
| Advantage | Constraint | Healthcare Impact |
|---|---|---|
| Tighter fit: Aligns controls closely with clinical workflows and specific cloud architectures. | Complexity: More segmentation can mean harder routing, firewall management, and troubleshooting. | Reduces blast radius for sensitive PHI while supporting time-sensitive clinical operations. |
| Cloud-native alignment: Uses policy-as-code and landing zones to automate compliance across hybrid and multi-cloud estates. | Resource demand: Needs platform engineering to build reusable modules without slowing release velocity. | Maintains a consistent security posture during telehealth growth or mergers. |
| Precision risk management: Allows for specific de-identification or tokenization strategies in research and analytics environments. | Cost: Cross-region replication and other high-resilience features can increase cloud spend. | Protects patient privacy in non-production environments without sacrificing data utility for research. |
| Vendor-specific controls: Enables granular vendor-specific risk assessments. | Inconsistent enforcement: Without strong governance, custom controls can fragment across teams. | Helps address third-party software risk, which accounted for 44.5% of initial access vectors in H2 2025 [1]. |
Custom frameworks give teams a level of fit that off-the-shelf models often can't match. The catch is simple: you need the time, people, and discipline to build and maintain them. Those tradeoffs come into sharper focus in the side-by-side comparison that follows.
Custom vs. pre-built: a direct comparison for healthcare leaders
Custom vs. Pre-Built Cloud Security Frameworks for Healthcare
Comparing compliance, speed, cost, and cloud depth
Side by side, the tradeoffs are much easier to see.
The biggest split comes down to who owns compliance mapping and evidence collection, a critical factor when you manage third-party risk across complex vendor ecosystems. That becomes a major issue when compliance pressure, cloud design, and team capacity are all pulling in different directions.
Pre-built frameworks come with mapped controls and third-party recognition. That can speed up audits, but it also narrows your room to maneuver. In plain terms, a prescriptive framework tends to work better in standard setups than in unusual ones.
Custom frameworks put the mapping work and evidence burden on your internal team. That means every control needs a clear link to a system, an owner, and an audit trail. A control isn't just a line in a spreadsheet. It has to connect to an asset, an owner, a change, and proof.
Cloud fit is another place where custom frameworks stand out. In complex setups, pre-built frameworks often need extra overlays to deal with provider-specific setups across AWS, Azure, and GCP. A custom model can account for those differences from day one. That matters when 73% of organizations operate hybrid cloud estates in 2026 [1].
When a hybrid approach works best
In practice, many mature healthcare organizations don't treat this as an either-or choice.
They use a pre-built framework for baseline governance, then add custom controls for edge cases. That gives teams third-party assurance for standard controls while keeping room for custom engineering in proprietary, multi-cloud, or clinical workloads. It can also help on cost: using multiple frameworks in a coordinated way can cut compliance costs by 40% through shared evidence and unified policies [6]. This efficiency is vital given the economic impact of third-party risk management on healthcare budgets.
That leads straight into rollout planning: scope, ownership, and evidence.
Comparison table: custom-built vs. pre-built frameworks in healthcare
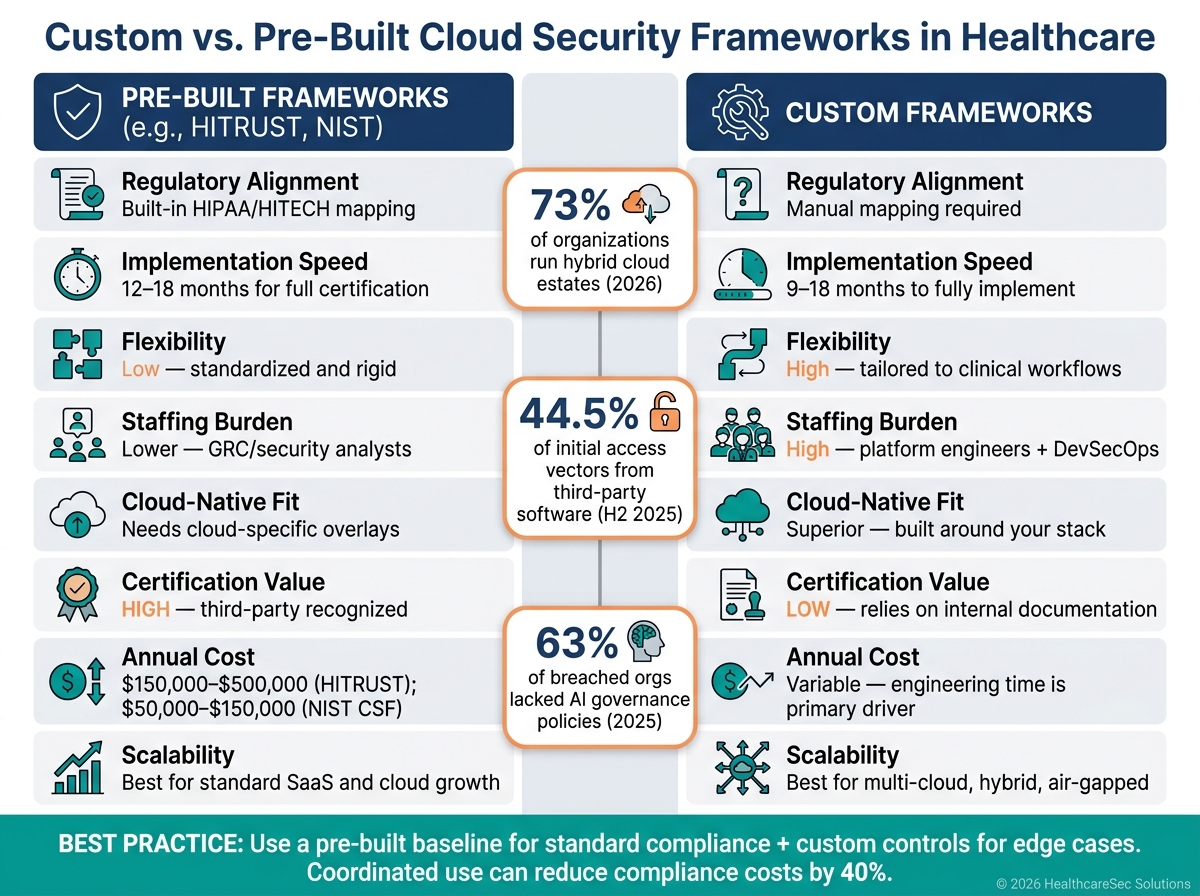
| Dimension | Pre-Built (e.g., HITRUST, NIST) | Custom-Built |
|---|---|---|
| Regulatory alignment | Built-in mapping to HIPAA, HITECH, and state laws [6] | Requires manual mapping and auditor justification |
| Implementation speed | 12–18 months for full HITRUST certification [6] | Slower; 3–6 months just to build the initial evidence pipeline [5] |
| Design flexibility | Low; standardized and rigid [6] | High; tailored to clinical workflows and legacy systems |
| Staffing burden | Lower; managed by GRC or security analysts [6] | High; requires platform engineers and DevSecOps expertise [1] |
| Cloud-native fit | Broad; often needs cloud-specific overlays [1] | Superior; built around your specific cloud provider stack [1] |
| Certification/attestation value | High; third-party certification reduces audit overlap [3] | Low; relies on internal due diligence documentation |
| Third-party assurance | Strong; reduces audit overlap across HIPAA, NIST, and ISO [3] | Lower without external assurance |
| Scalability | High for standard SaaS and cloud growth | High for multi-cloud, hybrid, and air-gapped environments [1] |
| Ongoing maintenance | Updates follow the framework provider and regulatory changes | Internal team updates controls for every regulatory or cloud change [5] |
| Annual cost range | $150,000–$500,000 (HITRUST); $50,000–$150,000 (NIST CSF) [6] | Variable; engineering time is the primary cost driver |
Implementation steps and conclusion: choosing the right model for your organization
Rollout steps for HDOs and healthcare vendors
The comparison table shows the tradeoffs. The next move is simple: turn that choice into a control model your team can run day to day.
Start with a current-state risk assessment. Look at threats and vulnerabilities across your cloud infrastructure, medical devices, third-party vendors, and supply chains while managing threats to patient care before you pick a framework [2]. Then choose one main reference framework based on your organization's risk profile: NIST CSF 2.0 for governance or HITRUST CSF for third-party assurance [1][4].
After you pick the baseline, map it to your actual cloud services and data flows. Tie high-level requirements to platform-native controls for key management, storage encryption, and secrets handling, with a focus on PHI, clinical workloads, and vendor-linked services [1]. Set up a responsibility matrix that spells out who owns each security duty across your team and each cloud service provider in IaaS, PaaS, and SaaS environments [2].
From day one, connect governance to remediation. Every failed control should have a named owner, a ticket path, and an SLA [1]. That way, issues don't just sit in a spreadsheet while everyone assumes someone else is handling them.
Once ownership and remediation are set, bring the workflow into one risk system. Censinet RiskOps™ centralizes third-party and enterprise risk assessments, evidence, and collaborative remediation for HDOs and vendors.
Key takeaways for making your final decision
The choice comes down to fit: compliance, cloud complexity, and operating capacity. Pick the model that lines up with your regulatory load, cloud setup, and the time and staff you have to manage it.
For many healthcare organizations, a hybrid model makes the most sense. Use a pre-built baseline for standard compliance, then add custom controls for edge cases. The aim isn't to pick the most ambitious framework on paper. It's to choose one your team can operate, evidence, and maintain over time.
FAQs
How do I choose between custom, pre-built, or hybrid?
Choose the setup that fits your priorities, engineering bandwidth, and timeline.
- Pre-built works best when you need to launch fast, your needs are fairly standard, and you want costs that are easier to plan for.
- Custom makes sense when you want maximum control and highly specific workflows, but it takes more time, money, and in-house skill.
- Hybrid gives you a middle path. You use pre-built core features, then add custom APIs or configurations where they matter most.
It also helps to weigh your risk tolerance and your total cost of ownership over 3 to 5 years, not just the upfront price.
Which framework is best for HIPAA and audits?
HIPAA is the legal baseline for U.S. healthcare organizations that handle protected health information. But here’s the catch: HIPAA does not offer a formal certification.
When organizations need to show compliance and get ready for audits, HITRUST CSF is often the go-to option because it maps HIPAA into a framework that can be certified. NIST SP 800-53 gives teams detailed controls that auditors can review, while NIST CSF helps organize and rank risks in a way that supports HIPAA compliance.
When is a custom framework worth the effort?
A custom framework is worth the effort when your security needs are highly specific. Think air-gapped environments, proprietary protocols, or medical device security that off-the-shelf frameworks don’t fully address.
It can also make sense when security is a core competitive edge, or when your scale makes vendor licensing and integration costs too high. In those cases, a one-size-fits-all setup can start to feel like forcing a square peg into a round hole.
Censinet RiskOps can help you manage both standard controls and your organization’s own requirements in one place.
